




Introduction
Specific driver genes are involved in the proliferation of lung cancer [1]. Various treatments have been developed to target these genes. For example, epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors and anaplastic lymphoma kinase (ALK) inhibitors have generated consistent responses in non-small-cell lung cancer with EGFR mutations and ALK translocations, respectively [2,3]. However, treatment responses to anticancer drugs show significant individual variations. Therefore, there is an unmet need to develop a reliable tool that can accurately predict treatment outcomes to determine appropriate therapeutic options. Patient-derived tumor organoids (PDOs) have emerged as reliable In vitro models that can predict drug responses [4,5]. Therefore, PDOs have been recommended as a precision medicine tool to choose an optimal treatment based on the tumorŌĆÖs genomic mutations in a clinical setting [4].
It is known that lung tumor organoids possess a similar tissue architecture to the parental tumor and maintain the genomic alterations of the parental tumor [6]. However, the current cancer organoid-based drug screening tests are inefficient and time-consuming. To develop a clinically useful assay, experimental studies have been conducted recently to evaluate the anticancer drug response of tumor organoids with microarray chips [7]. Drug response evaluation using a tumor organoid together with a microarray chip showed faster results than using only a tumor organoid. Here, we report a case of a rapid drug sensitivity test within 72 hours using tumor organoids that recapitulated the patientŌĆÖs response to anticancer drugs. This report was described according to the CARE guidelines for case reports.
Case Report
Ethical statements: This study was exempted from review by the Institutional Review Board (IRB) of Catholic Medical Center (IRB No: KC18TNSI0033). Written informed consent was obtained from the patients to participate in the study.
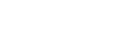
Patient information: A 50-year-old man visited The Catholic University of Korea, Seoul St. MaryŌĆÖs Hospital (Seoul, South Korea) on December 11, 2017, for the evaluation of an incidentally found right upper lobe (RUL) pulmonary nodule (Fig. 1). He was asymptomatic non-smoker and had no notable history of toxicological exposure, and there were no anomalous findings in his family medical history.
Clinical findings: No abnormal findings were seen in the initial physical examinations.
Diagnostic assessment: No distant metastases were found on brain magnetic resonance imaging (MRI) and positron emission tomography/computed tomography scans performed to confirm the patient's lung cancer stage before surgery. The mass was removed by thoracoscopic RUL lobectomy on January 10, 2018. Postoperative pathology confirmed a stage Ib (pT2aN0M0) poorly differentiated carcinoma, according to the 8th American Joint Committee on Cancer staging system. Moreover, lymphatic and vascular invasion were found. An EGFR mutation test was performed on the biopsy sample, and an exon21p.L858R mutation was detected.
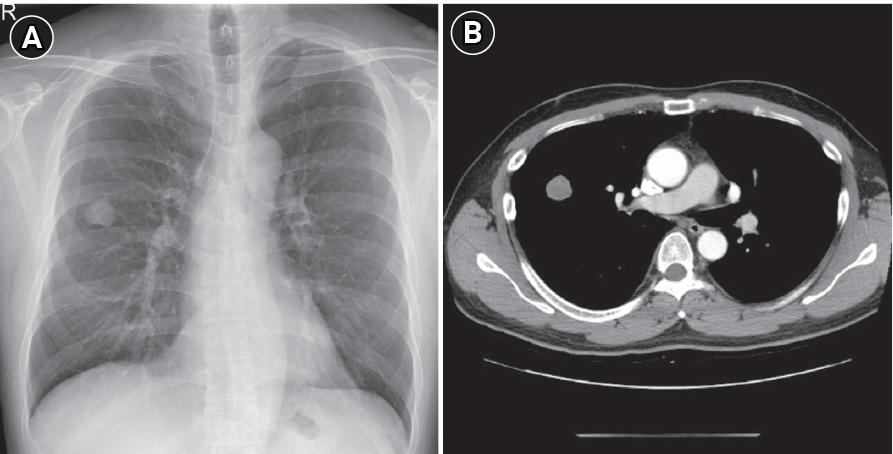
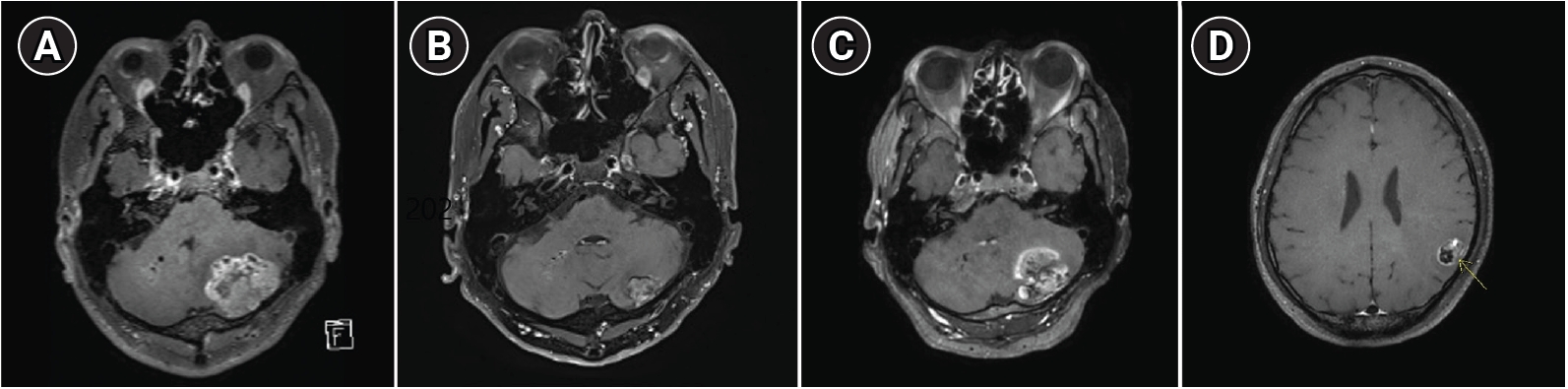
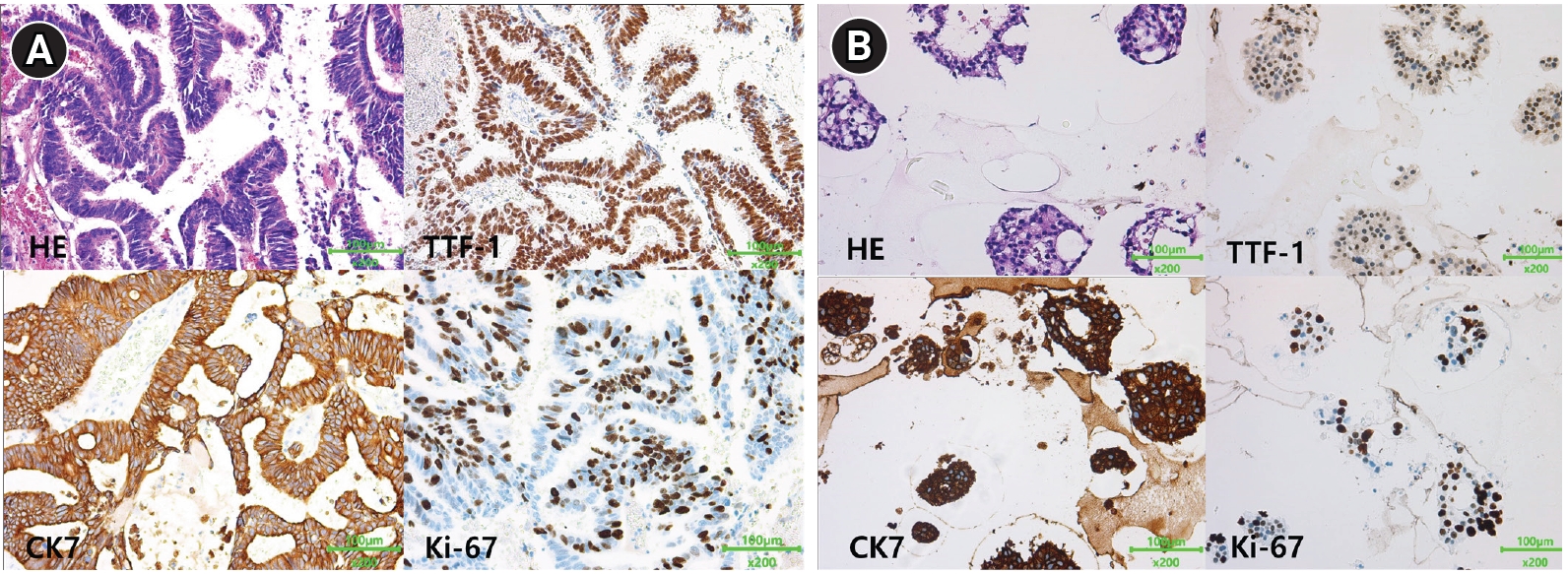
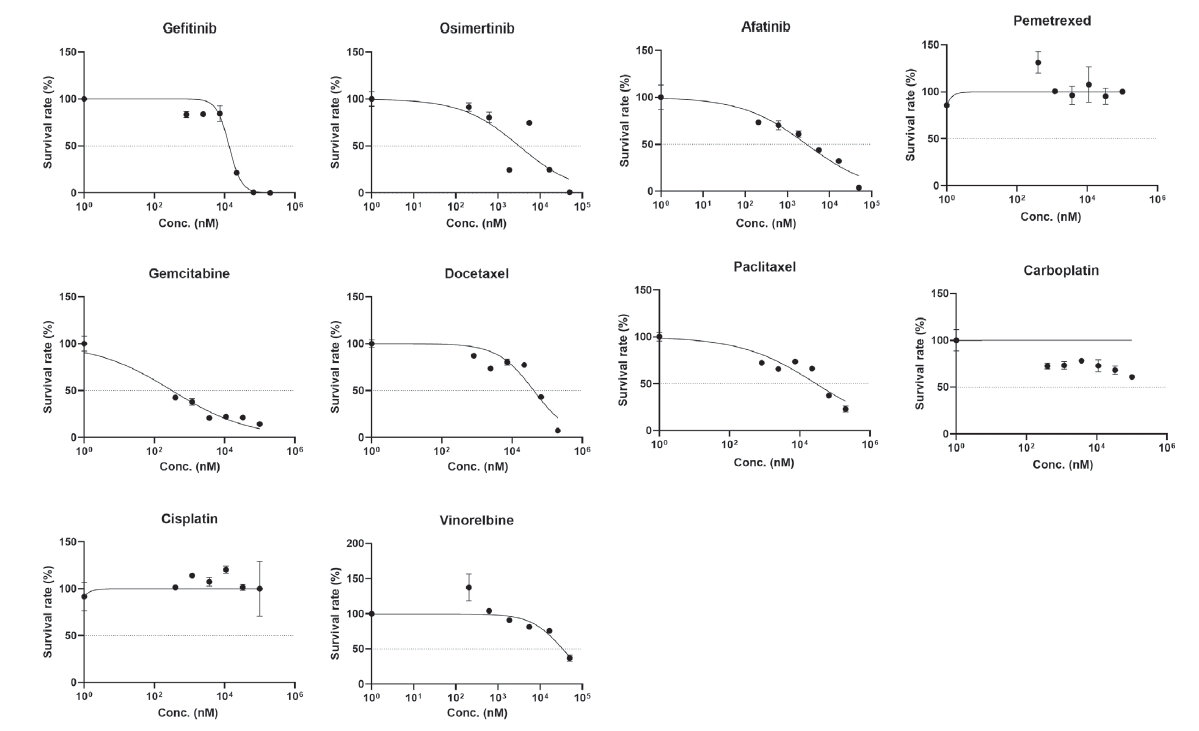
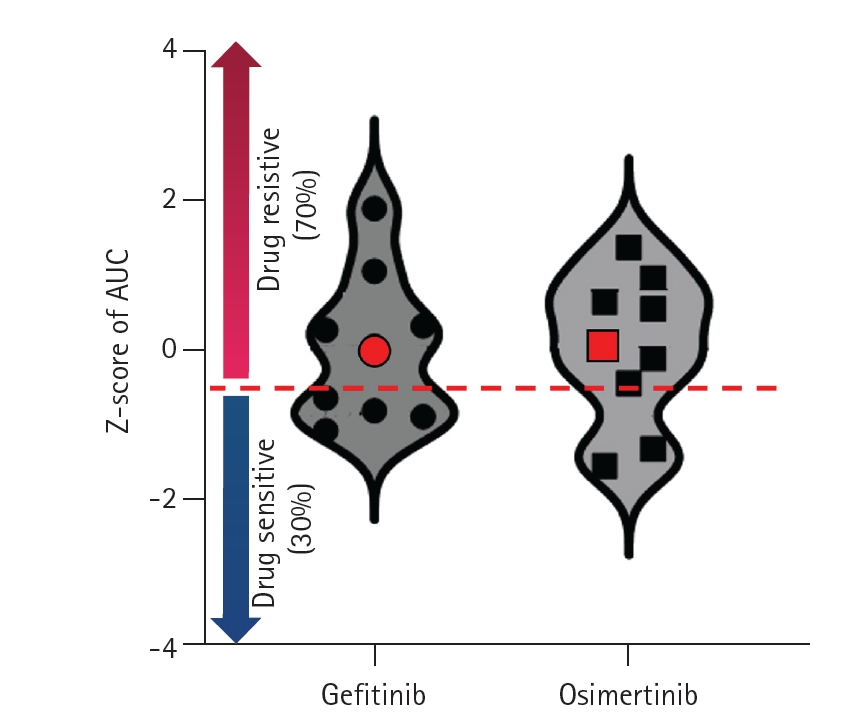
Therapeutic intervention and timeline: This patient received 4 cycles of adjuvant chemotherapy after surgery and was regularly followed up at an outpatient clinic. Brain MRI performed 17 months after surgery showed left cerebellar metastasis (Fig. 2A). The patient received intensity-modulated radiation therapy with gefitinib based on the previously confirmed EGFR mutation, and the brain lesion decreased in size after treatment, showing partial response (Fig. 2B). While taking gefitinib, the patientŌĆÖs aspartate aminotransferase (AST) level rose to 7 times higher than the normal range. The tyrosine kinase inhibitor was changed from gefitinib to erlotinib. Thirty-three months after surgery, growth of the left cerebellar metastasis was noted on a brain MRI examination conducted to evaluate the treatment response (Fig. 2C). The patient underwent craniotomy with left cerebellar tumor removal in 34 months after lung cancer surgery. Two EGFR mutations, exon21p.L858R and exon20p.T790M, were detected in the brain metastasis tissue. Erlotinib treatment was switched to osimertinib. Despite the change to osimertinib, a new brain metastasis was revealed on MRI (Fig. 2D) after 7 months. Fig. 3 summarizes the patientŌĆÖs clinical course (Fig. 3). PDO culture was performed from this resected brain metastatic tissue. The tumor sample was cultured in modified airway organoid medium (Cellvitro; Thermo Fisher, Waltham, MA, USA) for 18 days. Immunohistochemistry staining revealed that the organoid had maintained the morphological and molecular characteristics of the primary tumor tissue. (Fig. 4). After single-cell dissociation of the cultured organoids from the patient, the presence of the same EGFR mutation (p.L858R) as in the parental tissue was confirmed. In order to build tumor organoids within a shorter period of time and to evaluate drug sensitivity promptly, the following method was used. After splitting the patientŌĆÖs primary tumor tissue, dissociation was performed, and 3,000 to 5,000 cells were loaded into a 384-pillar chip for drug screening. Next, cells were cultured in the pillars for 3-5 days and observed with light microscopy. Once it was determined that organoids had formed, anticancer drugs were administered immediately after culture, and susceptibility to multiple anticancer drugs was evaluated by cell viability using calcein fluorescence staining and a cell titer with a three-dimensional assay after 3 days. For 10 anticancer drugs, the survival fraction of tumor cells according to drug concentration was statistically analyzed, and area under the curve values were calculated for each drug (Fig. 5). We prepared a distribution map of drug susceptibility using tumor organoids derived from 9 other previous patients. In the drug sensitivity distribution diagram, this case showed resistance to gefitinib and osimertinib (Fig. 6).
Follow-up and outcomes: This anticancer sensitivity profile in PDOs was correlated with patientŌĆÖs actual clinical response. He underwent 2 additional operations to remove brain metastases, and the transition to small cell carcinoma was confirmed during the final surgery.
Discussion
Historically, various systems have been developed to predict the clinical outcomes of anticancer drugs for patients. This includes two-dimensional cancer cell lines, patient-derived xenografts (PDXs), and PDOs [6]. Cancer cell lines can be used for high-throughput screening of anticancer drugs and provide facile prediction of anticancer drug responses; however, their clinical relevance remains highly controversial due to genetic differences during culture and limitations in simulating tumor heterogeneity and the microenvironment. PDXs are alternative models for predicting the drug response. They are established by the implantation of human tumor cells in immunocompromised mice [6,8]. PDXs could provide more reliable information on anticancer drug responses than cancer cell lines, but generating PDXs is a time-consuming and expensive process [6]. This prevents PDXs from being efficiently used in high-throughput anticancer drug screening.
PDOs have emerged as powerful In vitro cancer models to address this issue. PDOs accurately predict anticancer drug sensitivity for individual patients [6]. However, the current PDO-based method requires a laborious and time-consuming process to generate results. In this case, we successfully established a method to shorten the anticancer drug sensitivity response evaluation to 72 hours using a newly developed culture medium. Furthermore, the established PDOs showed genetic consistency with the patient. Moreover, the drug sensitivity test was correlated with the patientŌĆÖs actual clinical response.
Future advances in PDOs, together with an improved understanding of immuno-oncology, are anticipated to establish a comprehensive In vitro anticancer drug screening system. This system will recapitulate the human tumor microenvironment by integrating human stromal and inflammatory cells. In the future, our newly developed PDO system can be used to provide accurate information on the most effective clinical options for anticancer drugs for individual patients [9].
Patient perspective: The patient agreed to the treatment plan he received after hearing the physicianŌĆÖs explanation.
In conclusion, we applied a novel method of using tumor organoid drug response to shorten PDO-based drug sensitivity test time to 72 hours. The drug response test results of PDOs were found to be consistent with the patientŌĆÖs actual clinical course. This case report describes the rapid prediction of the tumor response in vivo to anticancer drugs and suggests the possibility of using this platform to screen multiple anticancer drugs and find the most potentially effective one in customized cancer treatment. A large-scale future study is warranted for further applications in real clinical settings.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






